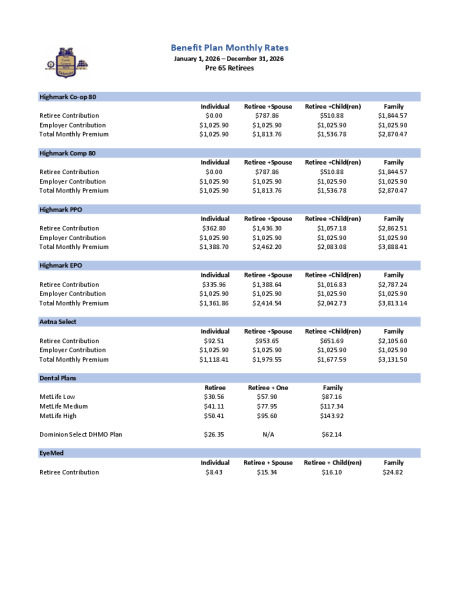
2026 Total Monthly Premium Rates Pre 65 Retirees
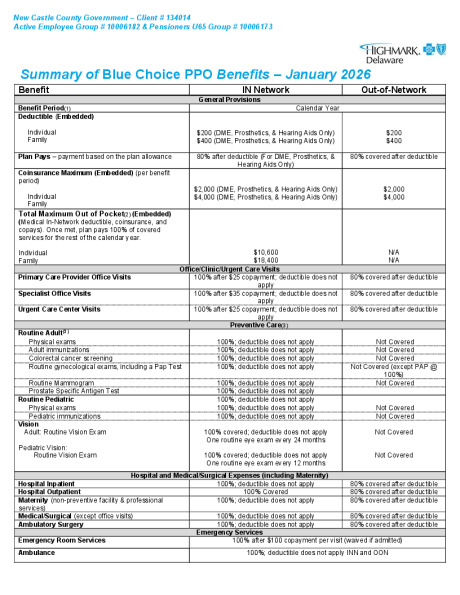
2026 Highmark Blue Choice PPO
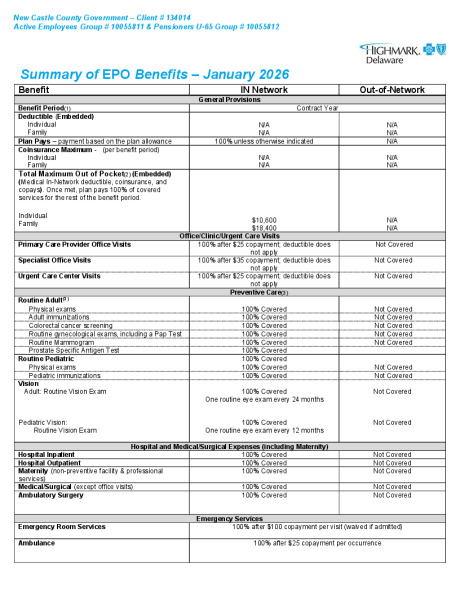
2026 Highmark EPO
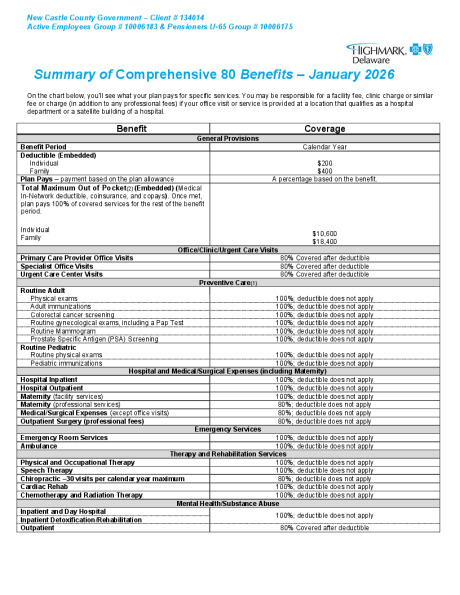
2026 Highmark Comprehensive 80
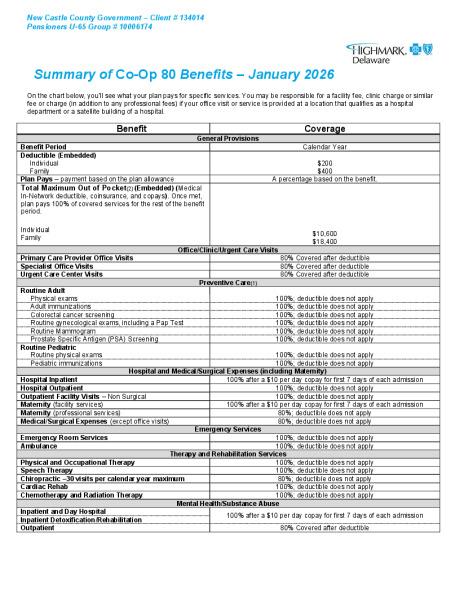
2026 Highmark Co-Op 80
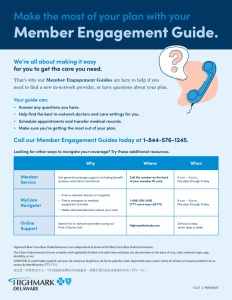
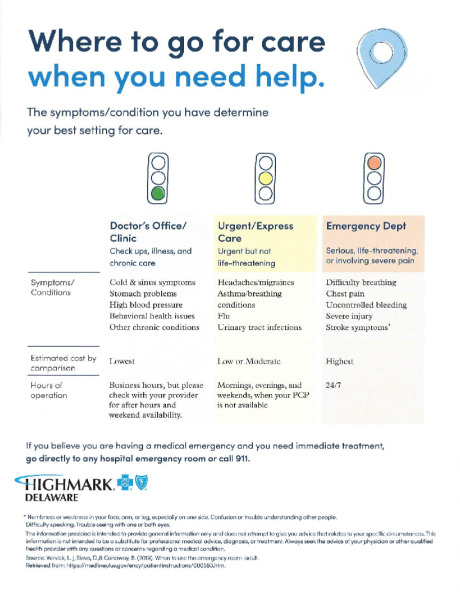
Highmark Urgent Care

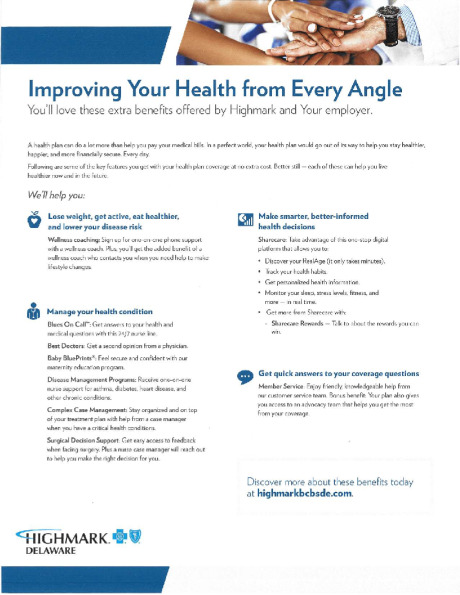
Highmark Coaching Program


Highmark Sword Campaign


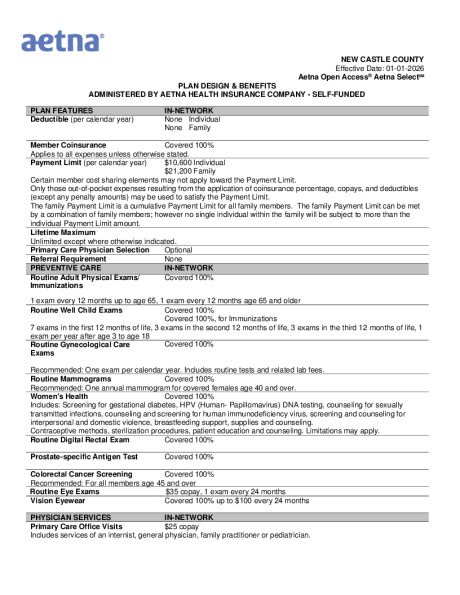
2026 Aetna OpenAcess Plan Summary

Aetna Health App
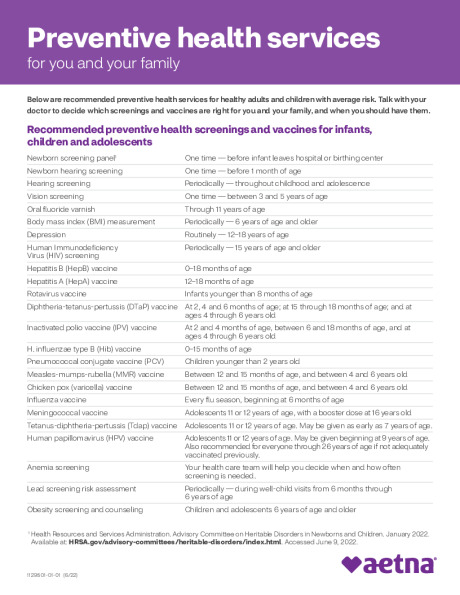
Preventive Care Schedule
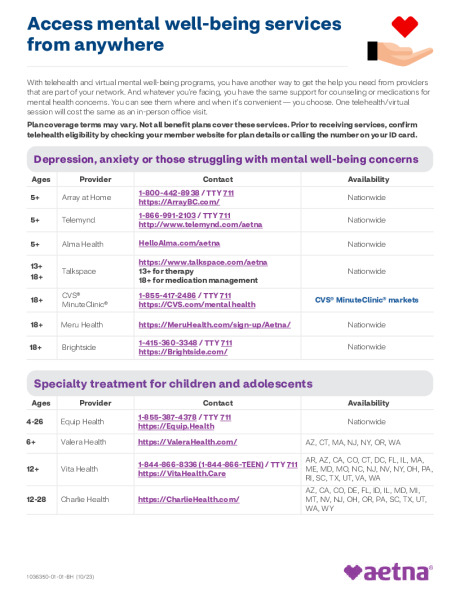
Behavior Health Programs and Services