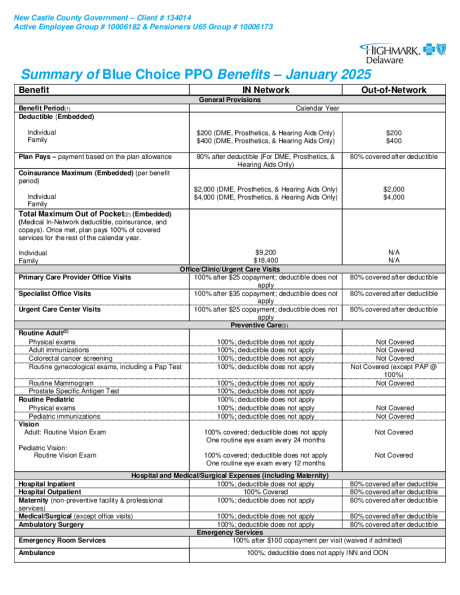
New Castle County - Blue Choice PPO - January 2025
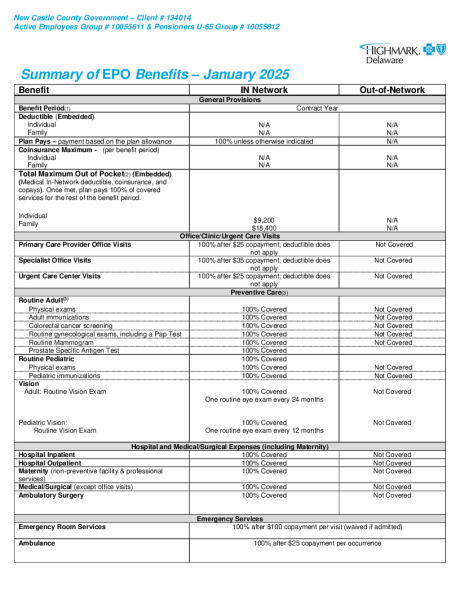
New Castle County - EPO - January 2025
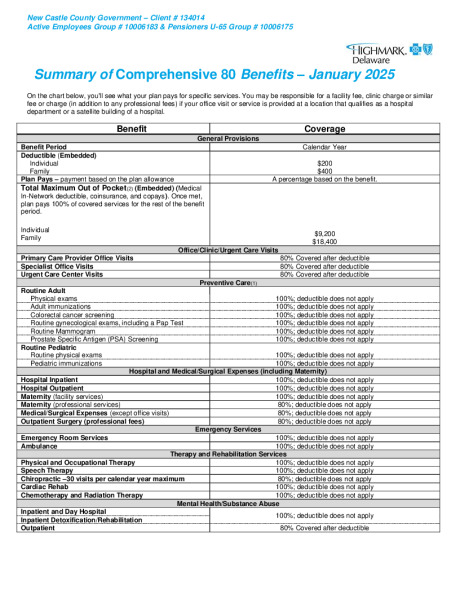
New Castle County - Comprehensive 80 - January 2025
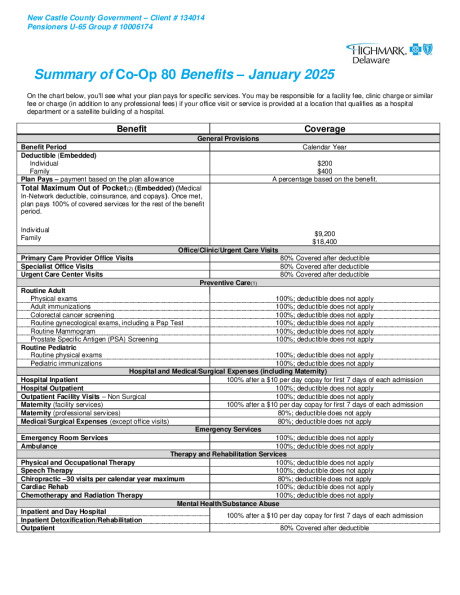
New Castle County - Co-Op 80 - January 2025
Highmark Coaching Program
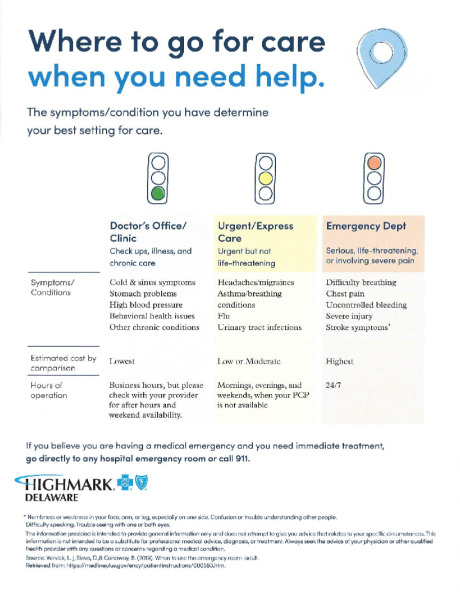
Highmark Urgent Care


Highmark Sword Campaign

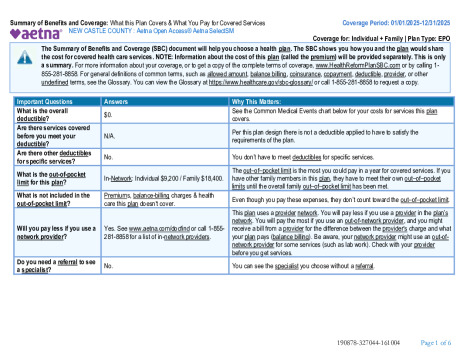
Aetna Select SBC 010125
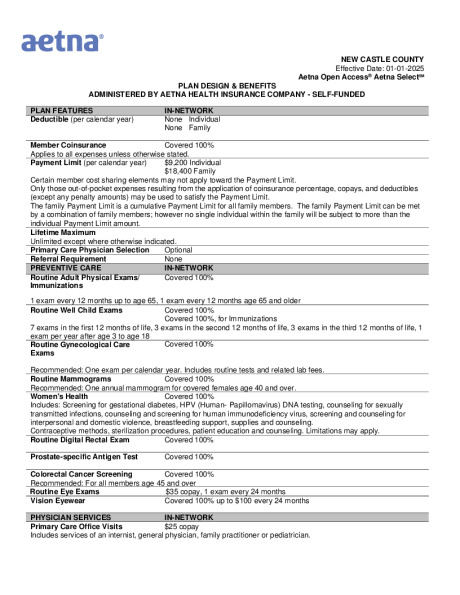
NCC_Aetna OpenAcess Plan Summary_010125

Aetna Health App
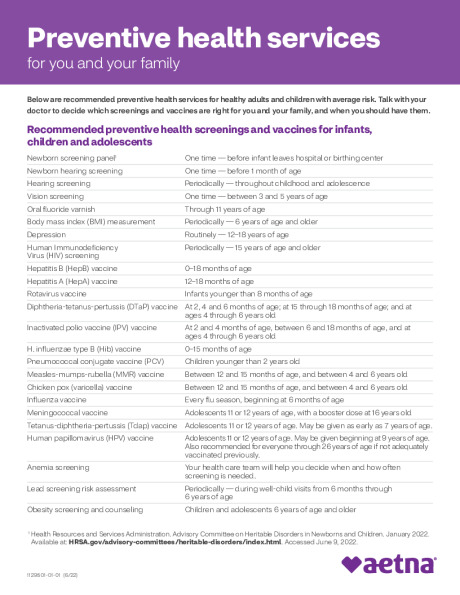
Preventive Care Schedule

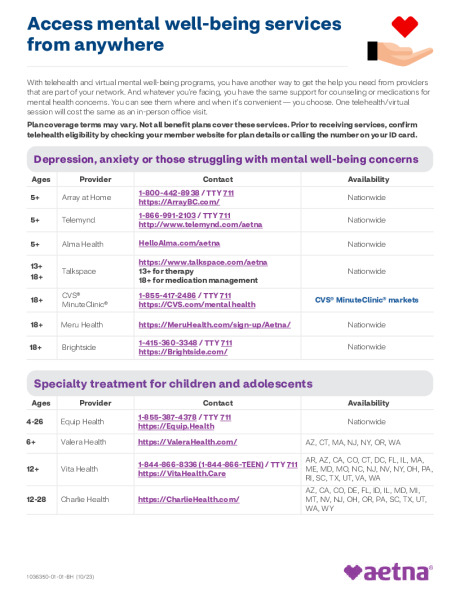
Behavior Health Programs and Services