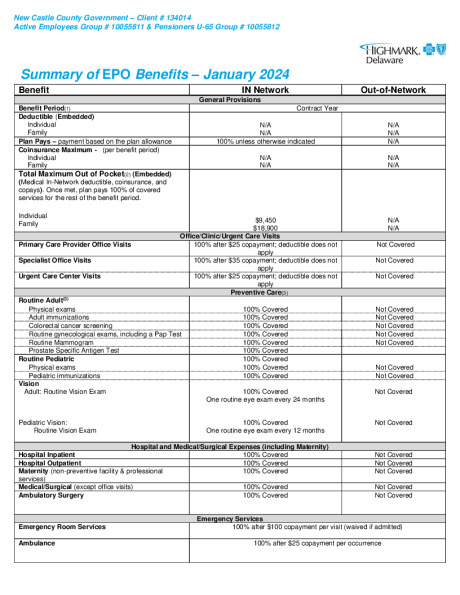
Highmark EPO
Highmark Coaching Program
Highmark Urgent Care


Highmark Sword Campaign


Aetna Health App
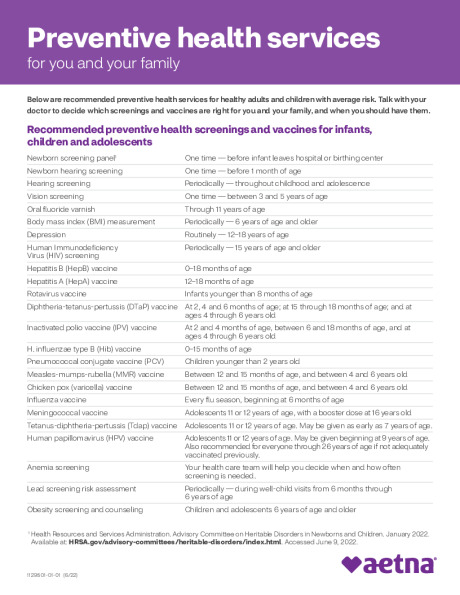
Preventive Care Schedule