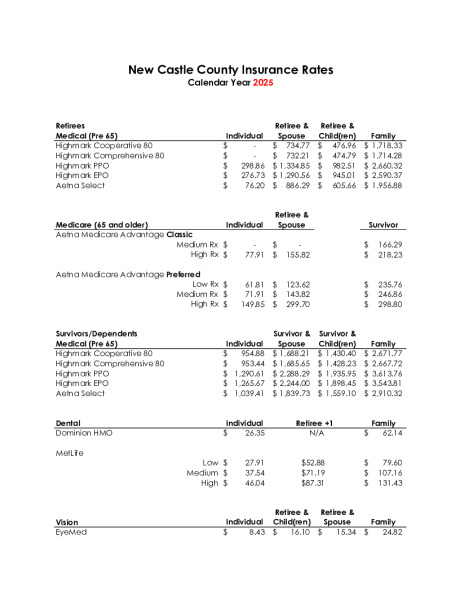
2025 Health Premiums For Pensioners
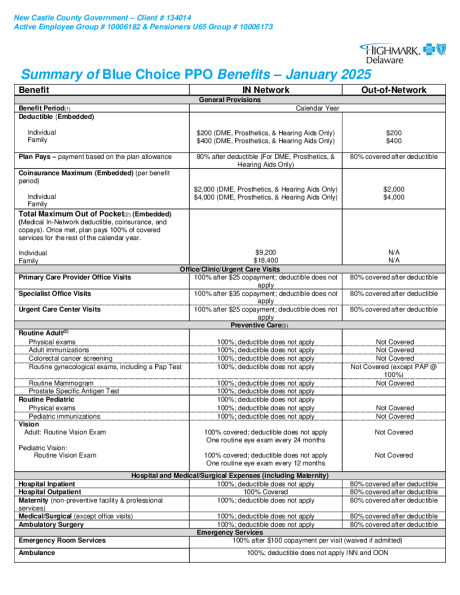
New Castle County - Blue Choice PPO - January 2025
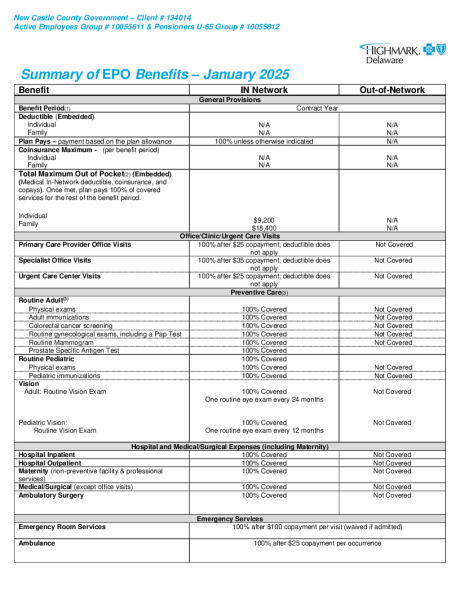
New Castle County - EPO - January 2025
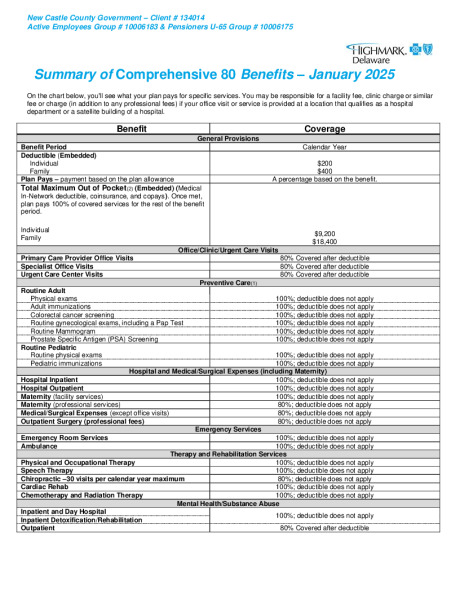
New Castle County - Comprehensive 80 - January 2025
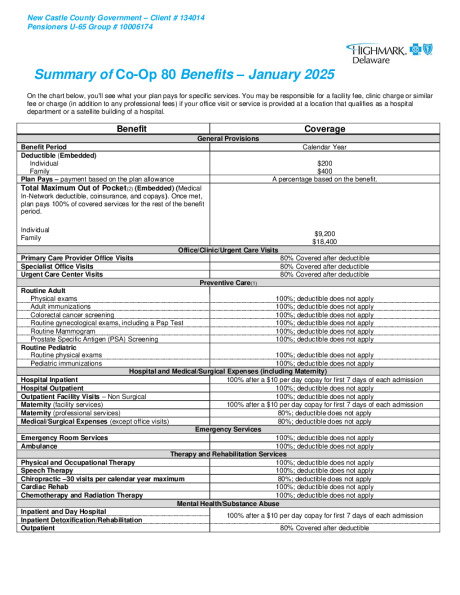
New Castle County - Co-Op 80 - January 2025
Highmark Urgent Care

Highmark Coaching Program


Highmark Sword Campaign


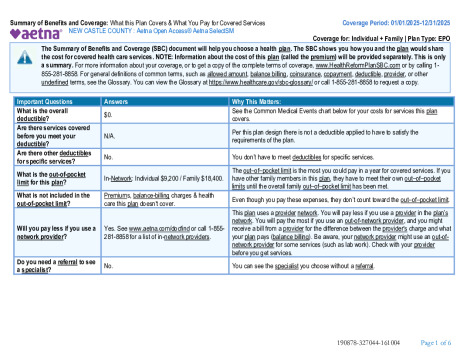
Aetna Select SBC 010125
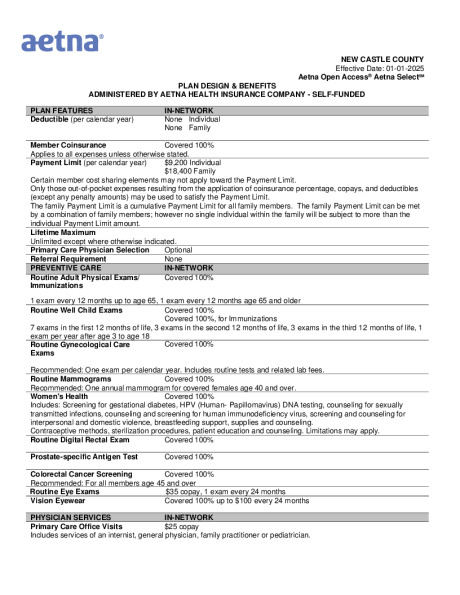
NCC_Aetna OpenAcess Plan Summary_010125

Aetna Health App
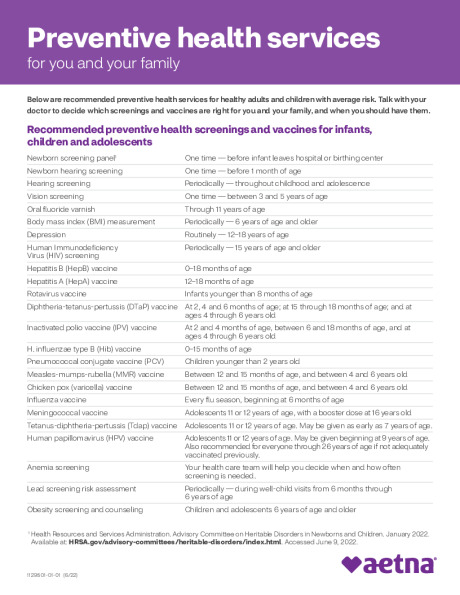
Preventive Care Schedule
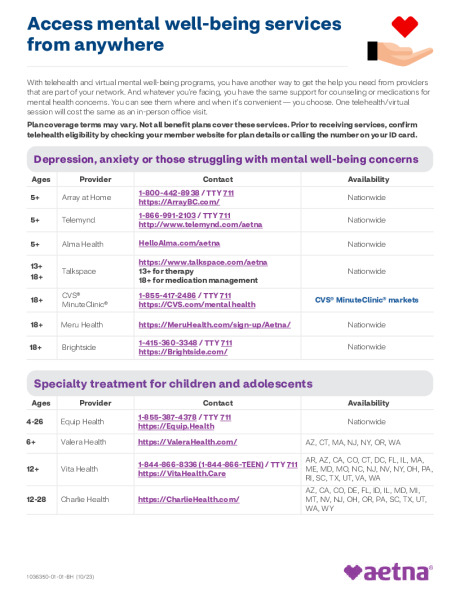
Behavior Health Programs and Services

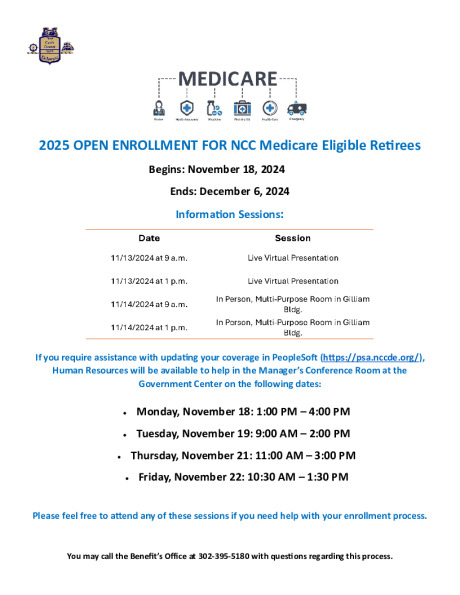
MEDICARE OPEN ENROLLMENT FLYER 2025
2025 New Castle County OE Presentation
2025 Health Premiums For Pensioners
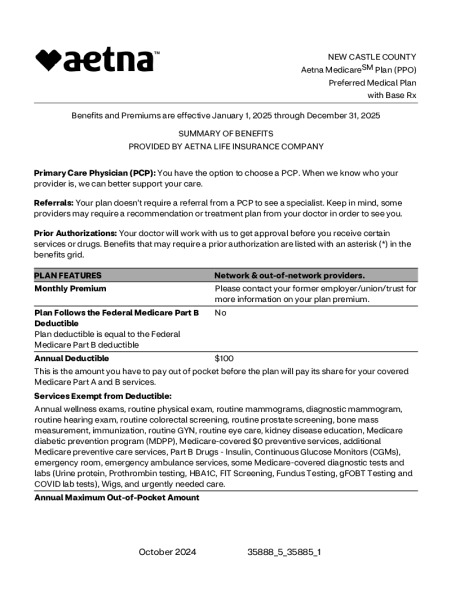
Preferred Medical with Base RX
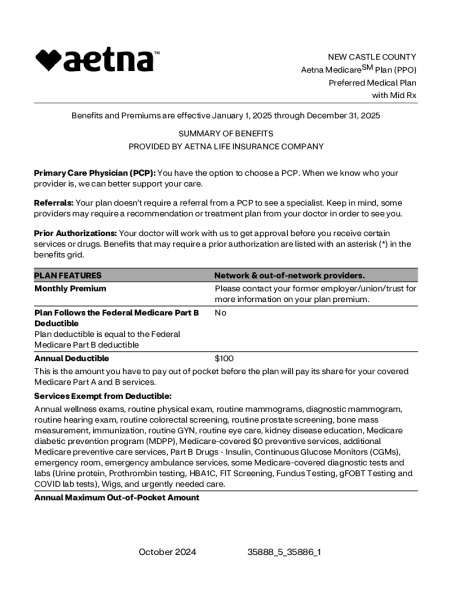
Preferred Medical with Mid RX
Preferred Medical with High RX
Classic Medical with Mid RX
Classic Medical with High RX


Get Active with SilverSneakers

Aetna Discount Program - Medicare Solutions
